 ndegendogo
commented
3 years ago
ndegendogo
commented
3 years ago So I think meaningful numbers to track "app performance" and acceptance could be:
- total number of downloads vs all people in this country. The misses are those who don't want it (after all, it is voluntary), or don't have the technical precondition (a smartphone that is not too old)
- number of people upgrading their version vs total downloads. afaik both Apple and Google shops track this number. The misses have deinstalled the app after initial download (out of frustration or whatever reasons).
- number of devices downloading the daily keys vs installations (or upgrades?). It shows 'active' users - actually: active devices, so this number is a bit tricky (if I use two devices on one account : one installation, but two active devices). The missing show issues with the daily check (although the check may even fail after the key download)
- number of DK upload (QR + teleTAN) vs active users / active devices
- share of teleTAN actually used for upload
- method of upload (QR vs teleTAN)
 alanrick
alanrick MikeMcC399
MikeMcC399 daimpi
daimpi coder66
coder66 Blackjacx
Blackjacx askozyreva
askozyreva pitsch
pitsch
 cfritzsche
cfritzsche mrs1959
mrs1959 heinezen
heinezen

 stweil
stweil dsarkar
dsarkar
 annebeckmann
annebeckmann


 Ein-Tim
Ein-Tim
{kind=link}
{kind=link}
{kind=link}
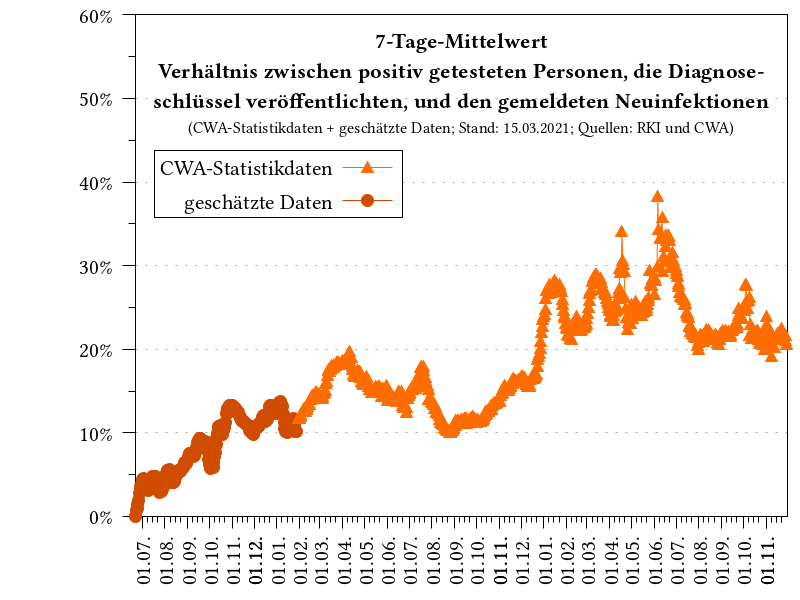
Zahlen:
Nimmt man alles zusammen ergibt sich, dass von 30.000 Infizierten statt 390.000 Schlüssel nur ca. 11.000 übermittelt wurden.
Damit liegt die aktuelle Nutzung der App bei ca. 2,8%.
Ich finde das sehr traurig und frage mich wo die Ursachen liegen und wie man dies ändern kann.
P.S. Da es nichts mit dem Code der CWA App zu tun hat, habe ich hier in Deutsch geschrieben.
Internal Tracking ID: EXPOSUREAPP-4916