 louisgv
commented
6 years ago
louisgv
commented
6 years ago -
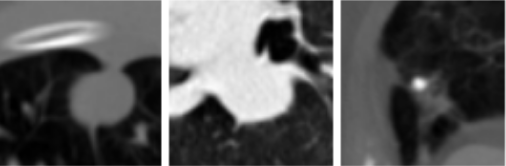
How often does radiologists spot error in patient's files/data and what kind of tool do they currently using to validate data and/or fix error? What kind/piece of data are most prone to error? (Looking at data provided in the RSNA specifically)
-
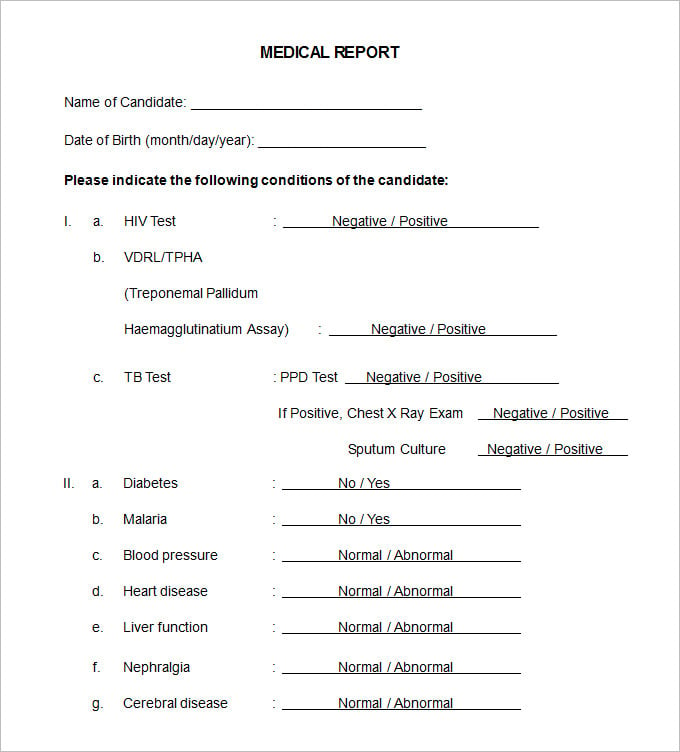
In the Report/Export view, would clinicians prefer to have as much data cramped into the view-port as possible (for quick scanning, for example) in a way similar to infographic report example or would they prefer spacial line-by-line document format example? (Specifically talking about the RSNA standard)
-
Is there a process to update a patient's record once it has been saved? If not, how long does it take to update patient record? If instantly, how long does it take to validate if the new data is correct? And how long does it take until patient's treatment get updated according to their new status?
NOTE: The 2nd question targets specifically for digital viewing. Exported file will be formatted to follow the formal convention.
 WGierke
WGierke musale
musale isms
isms hengrumay
hengrumay lamby
lamby vessemer
vessemer


 swarm-ai
swarm-ai eelvira
eelvira kyounis
kyounis{kind=link}
{kind=link}
This project is about making something useful for clinicians. This is your chance to pull up and get input from radiologists working on the front lines of early detection. We would love to hear what you are wondering about in terms of the workflow at the clinic, and where user input can address thoughts that are coming up for you as you work on the application.
The team at ALCF will be coordinating responses to submitted questions through their network of clinicians, researchers, and patients.
Submit a question by commenting directly on this issue. You'll earn 2 community points for each of up to three original, substantive questions.