 mgranberryto
commented
7 years ago
mgranberryto
commented
7 years ago I have been using the referenced Novorapid (Novolog) curves, using Humalog insulin and dia=5, live for about 12h and have found a much better correlation with observed data over the last 2 weeks than I had with the old formulas. My modification to calculate.js, based on Tim's work, is available here: https://gist.github.com/mgranberryto/e5116dbc314cdf78513f4d185684b8a5
 sulkaharo
sulkaharo tim2000s
tim2000s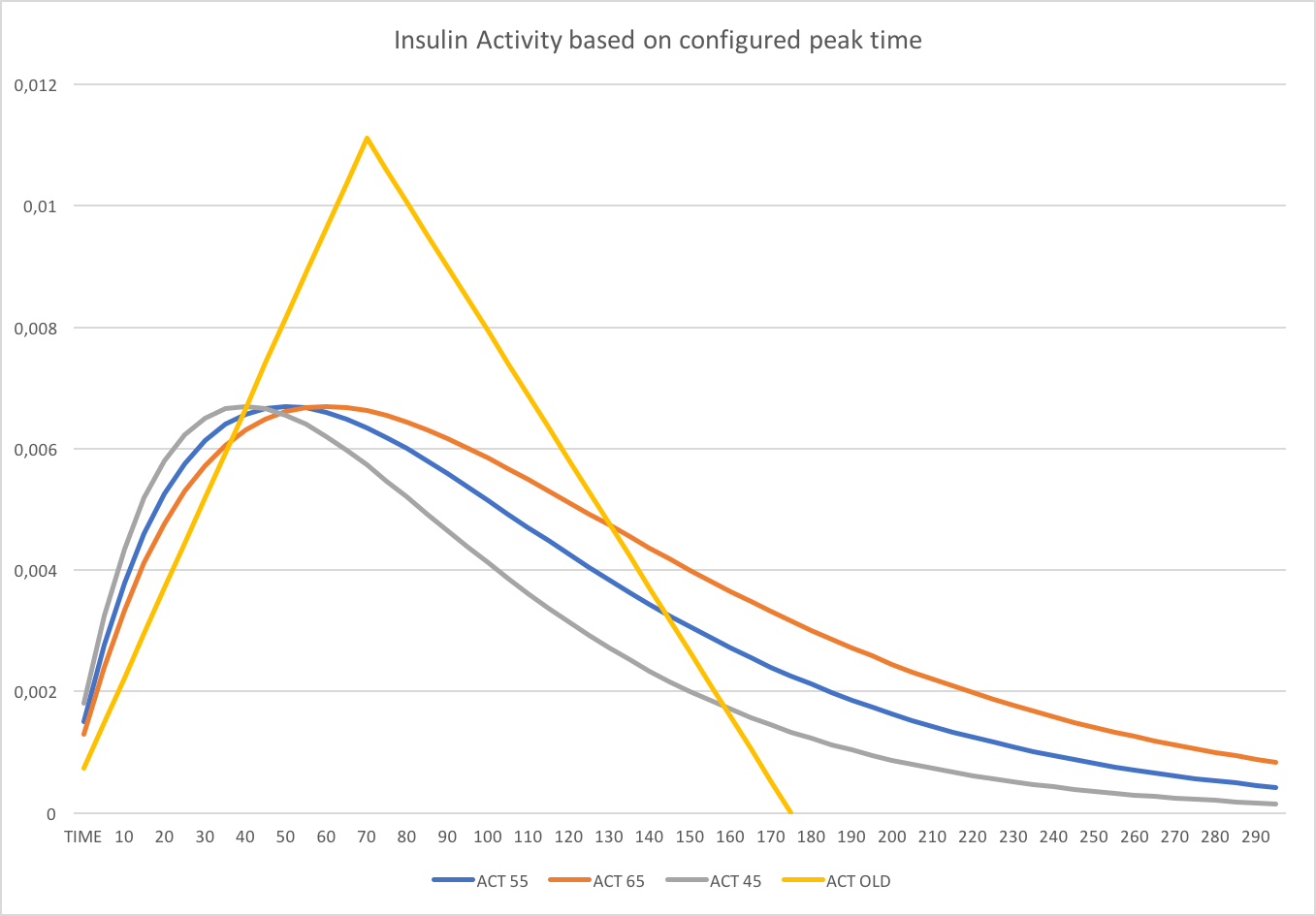

 tepidjuice
tepidjuice scottleibrand
scottleibrand PieterGit
PieterGit ghost
ghost rdsteed
rdsteed cjo20
cjo20 efbest
efbest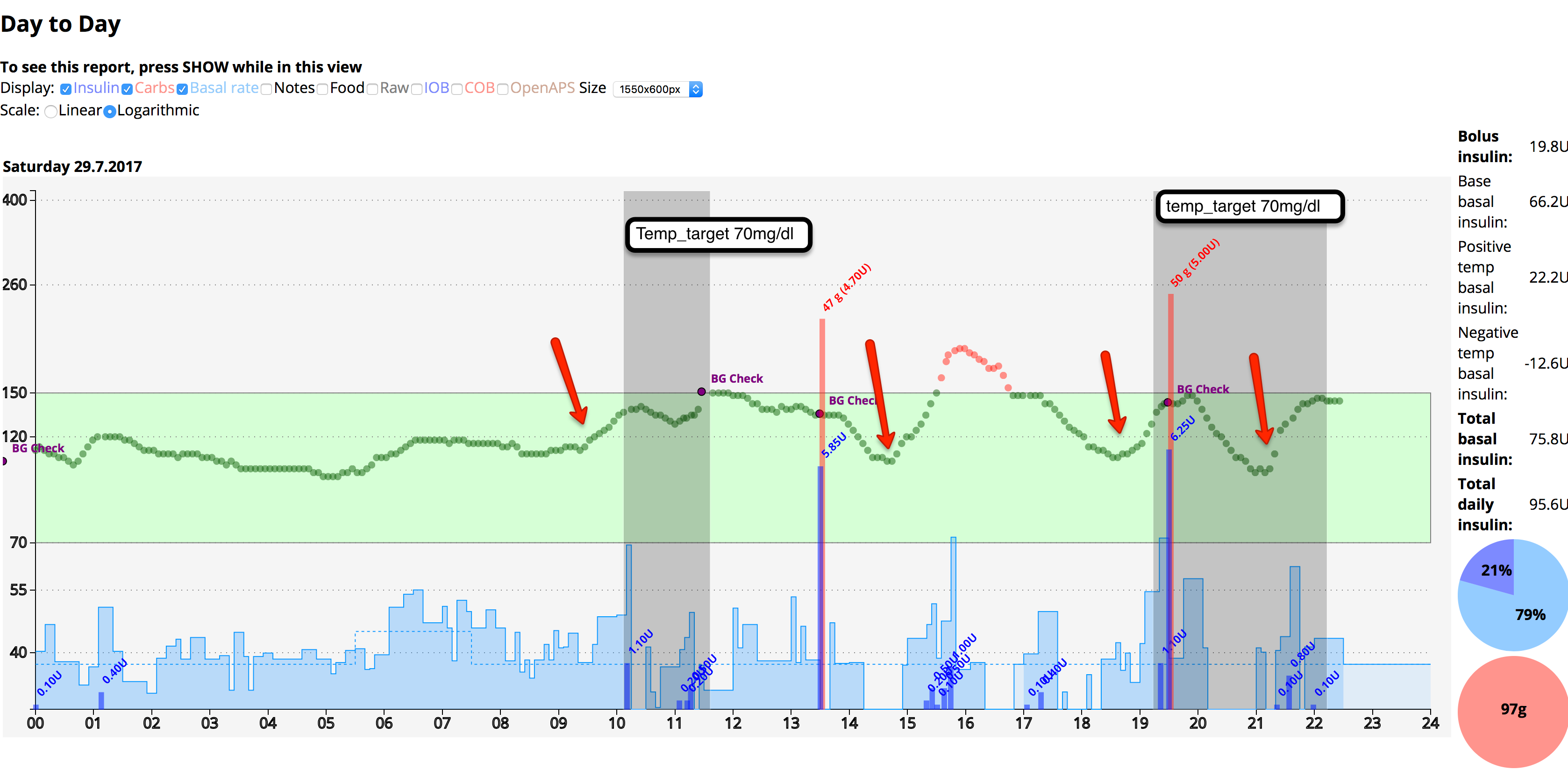
Enhancement to iob/calculate.json to use real curves and allow a choice between Fiasp and standard fast acting during set-up.
The curves are available at https://github.com/LoopKit/Loop/issues/388
Potential issues include variation in peak time when scaling curves by DIA and when to cut off action.
Also question whether we should have standard curves by default and require an enable flag to swap those out for fiasp or whether it should be included in the interactive setup.
I'll submit a branch to allow users to test my Fiasp curves once tested over the weekend, but no setup configuration work has yet been done.